
A National Seniors Strategy Needs to Account for Complexity in the Aging Process
Russell Williams
A national seniors strategy cannot be based solely on age. Stratification based on risk and health resource utilization is also required. Importantly, a strategy must consider those with frailty. Frailty places large burdens on health and social care systems, as well as on family/friend caregivers, including financial, social and productivity costs. Everyone is impacted by frailty. There is a pressing need for systems reform that accounts for the complexity of the aging process and offers more integrated, patient-focused, preventive care options.
We are succeeding in shifting the aging curve through preventive interventions and better public health. In the 2016 Census, people 65 years and older outnumbered children 14 years and under for the first time, which means our needs, as a society, are changing.
There are many calls for a national strategy for seniors, and for home-care, palliative care, dementia and pharmacare strategies, which will impact care for seniors. However, any strategy targeting seniors cannot be based solely on age. Stratification based on risk and health resource utilization is also required.
Media images of healthy seniors continuing with all their activities are misleading. Not everyone ages in the same way and aging does increase the odds of developing chronic medical conditions, or frailty.
Clinical frailty can occur at any age and describes individuals who are in precarious health, have significant multiple health impairments, and are at higher risk of dying. The hallmark of frailty is that minor illnesses like infections or minor injuries, which would minimally affect non-frail individuals, may trigger rapid and dramatic deterioration in health.
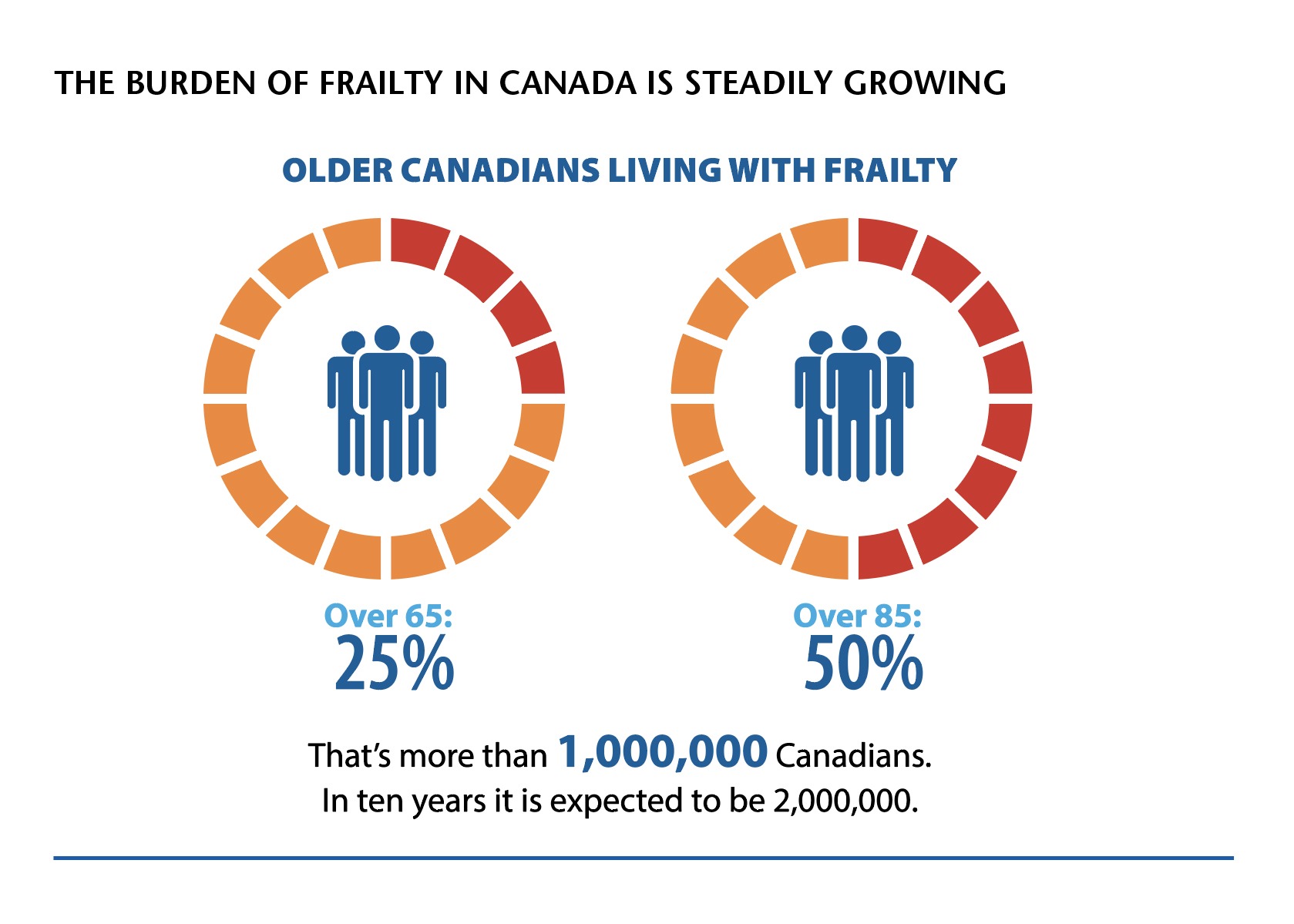
Getting older doesn’t necessarily mean you are frail. It does mean that as you age you are more likely to become frail. Frailty is a more precise, and evidence-based, determinant of health outcomes and health care utilization than age alone. The most rapidly increasing segment of the population is individuals over 80 years old and over 50 per cent of those over the age of 80 are frail.
A large, growing proportion of our health and social care spending is, and will increasingly be, focused on older Canadians living with frailty. From a societal perspective, frailty also places large burdens on family/friend caregivers, including financial, social and productivity costs. Everyone is impacted by frailty.
 Our health care system evolved several decades ago when people generally died younger and with a “single system” illness. In terms of social supports, many people lived in intergenerational households or close to family who could help them live independently. Today, our health and social support systems scramble to meet the needs of older people with multiple, simultaneous, and often inter-related health and social issues that threaten their independence.
Our health care system evolved several decades ago when people generally died younger and with a “single system” illness. In terms of social supports, many people lived in intergenerational households or close to family who could help them live independently. Today, our health and social support systems scramble to meet the needs of older people with multiple, simultaneous, and often inter-related health and social issues that threaten their independence.
Frailty is poorly understood, pervasively under-recognized, and under-appreciated by health care professionals and the public. Not enough health care professionals have expertise in caring for older adults that live with frailty, and we do not have sufficient evidence to guide the care of older adults living with frailty.
The problem is that many therapies, treatments and care strategies have only been studied in people who are not frail. As a consequence, we don’t know if current therapies are beneficial or cause harm, are cost-effective, or waste scarce health and social care resources in those living with frailty. Without evidence, aggressive and expensive technologies are often overused without improving outcomes, causing undue suffering for patients, undue distress to their families, and wasted health care resources, threatening the sustainability of our health care system.
The bottom line is that our health and social care systems are challenged to improve the quality and quantity of care delivered to older Canadians living with frailty.
The Canadian public is cognizant that not all aging is the same and some seniors need more support. There will be increasing pressure from the baby boomer generation who are now caregivers and in some cases becoming frail themselves. They are also politically savvy and have proven themselves to be strong advocates for causes that matter to them.
What does this mean for the Canadian health and social care systems?
Public pressure may finally catalyze change in health care systems and policies, and in social supports for seniors. Any national strategy that impacts seniors and their families must bring together all groups that have a role to play, and must take into consideration varying needs, in particular frailty. As Canada’s sole organization devoted to improving care for older Canadians living with frailty and supporting their family/friend caregivers, the Canadian Frailty Network (CFN) is positioned to contribute to this strategy.
CFN’s work centres around increasing frailty recognition and assessment, providing evidence to inform decision making from the bedside to policy making, training the next generation of care professionals and scientists, and mobilizing knowledge to catalyze change in health and social care systems. All settings of care are covered, from acute and critical care to community care, and including end-of-life care and advance care planning.
What would transformed health and social care systems look like if frailty were considered?
Older adults living with frailty and their family/friend caregivers would be involved at every stage of system changes—from planning to implementation to evaluation. When citizens are engaged in decision making, it improves the patient experience, contributes to more cost-effective services and enhances the overall quality of our health and social care systems.
The Canadian Frailty Network undertook a study aimed at identifying priority areas based on input from Canadians affected by older adults living with frailty. The two top priorities identified dealt with 1) better organization of health and social care systems to provide integrated/coordinated care, and 2) tailoring care, services and treatments to meet the needs of older adults who are isolated or without family/caregiver support or advocates.
Identification and assessment of frailty would be standard clinical practice in care settings across Canada. Older adults who come into contact with the health system and who meet pre-specified criteria would be assessed for frailty, with the type of assessment being determined by the situation. Results would be captured and shared through electronic medical records, like the work CFN is collaborating on with Fraser Health (CARES program), the University of British Columbia and the Canadian Primary Care Sentinel Surveillance Network (CPCSSN) which will help primary care practitioners identify and treat those who are frail.
There would be common data collection, measurement and coding across health and social care systems, which would be shared between care providers, and accessible to researchers. Researchers would collect common data elements and report on common outcome measures; a major initiative underway by Canadian Frailty Network, working with international groups such as interRAI.
Training and certification qualifications for caregivers and health care professionals would include frailty recognition and assessment; a paradigm shift in how we are training people to equip them for health and social care with the skills they need. One of CFN’s key activities has been our interdisciplinary training program targeted to frailty. More than 850 young scholars, students, trainees and working professionals have developed and enhanced specialized skills and advanced knowledge to provide the best evidence-based care.
Research on frailty would be a priority for funding, with increased evidence for policy and practice decision making. Canada is a leader in frailty measurement, with Canadian researchers (and CFN Network Investigators) pioneering some of the most commonly-used tools, such as the Clinical Frailty Scale and the Edmonton Frailty Scale. Unfortunately, Canada has been comparatively slow to adopt its own innovations, lagging behind other nations; CFN is reversing this trend. CFN has galvanized the Canadian research community to focus on frailty with an investment of $20.59 million, including partners, which has led to $12.76 million in follow-up investments from external funders.
More integrated models of health care would recognize social determinants can be as important as medical interventions and would embrace rehabilitative and social supports to improve care and quality of life. Care planning would recommend evidence-based interventions related to specific measures of frailty, and these would include non-medical interventions (like many funded by CFN) to address things like nutrition, exercise and mobility, advance care planning, oral care and social isolation.
Innovative approaches to residential care needs would help seniors remain in the community as long and as independently as possible, including those who live with frailty. Care planning would consider patients’ personal values during clinical care, and during transitions of care—what is most important to patients in their daily lives, including where they reside.
Caregivers would be supported to ease the economic and other burdens of home care. Support for caregivers of older adults has been shown to reduce institutionalization, hospitalization and readmission. Effective interventions provide education and skills training, respite and self-care for the caregiver, and economic support.
Transforming health and social care systems to incorporate frailty will produce significant societal and economic benefits. The need for system change is real and significant for older Canadians, their families, and for those on the front lines delivering care.
Crafting a national strategy within Canada’s multi-jurisdictional system is a complex policy challenge requiring a multi-faceted perspective, clarity, and a desire among stakeholders and leadership to collaborate. And, the will to act.
Russell Williams is Chair of the Board of Directors of Canadian Frailty Network and Vice President, Government Relations and Public Policy, at Diabetes Canada. boardchair@cfn-nce.ca